What’s Up With Shoulder Impingement?

One of my favorite Instagram accounts is @chicagosportsdoc. I know you’ll geek out on this if you’re into anatomy, but you may want to finish lunch before browsing.
But sorry, I do need to show you one thing…
I remember saving the following post, not because of the image but because of what happened in the comment section.
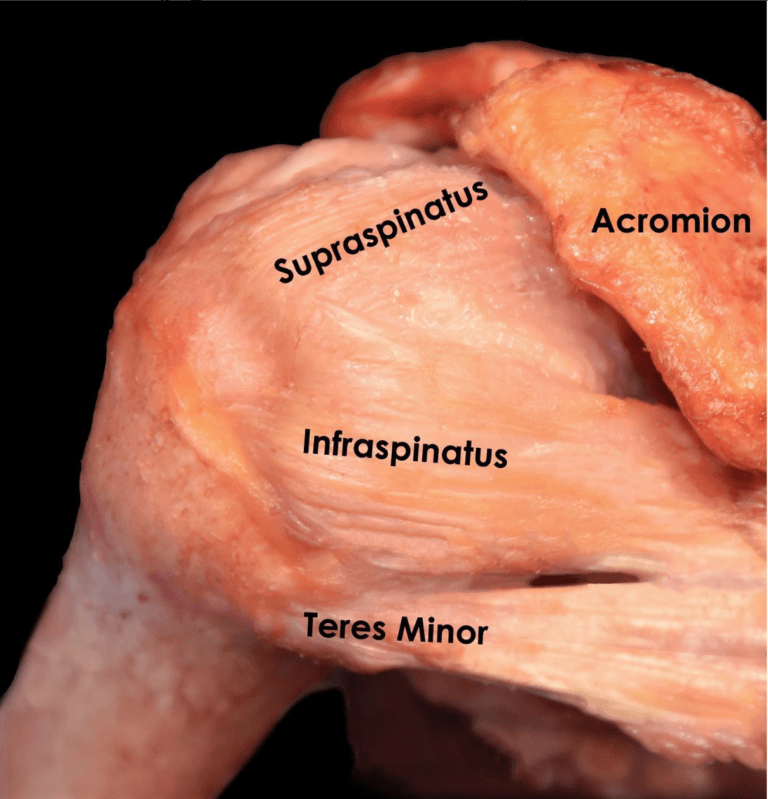
Here we have a renowned surgeon who operates on multi-million dollar athletes, spent more than a decade studying his craft, and seems to toy around with cadavers in his free time, referring to a typical ailment called shoulder impingement.
Yet, some of the responses sought to inform him that shoulder impingement is not a real thing?
So, it appears there is some controversy. Especially when PubMed turns up about 300 articles from the last two years containing the term “subacromial impingement,” and almost all of them (other than a few opinion pieces) still point to pinching under the acromion as the culprit.
But the shoulder impingement nay-sayers aren’t just a bunch of conspiracy theorists. There is good evidence that the acromion isn’t such a bad guy regarding shoulder problems.
So I’ve decided to take the new few newsletters to dive into the current state of shoulder impingement.
WHAT IS SHOULDER IMPINGEMENT?
In 1972 the surgeon Charles Neer published a paper blaming the bony structure that sits over the shoulder, called the acromion process, as the primary cause of shoulder pain.
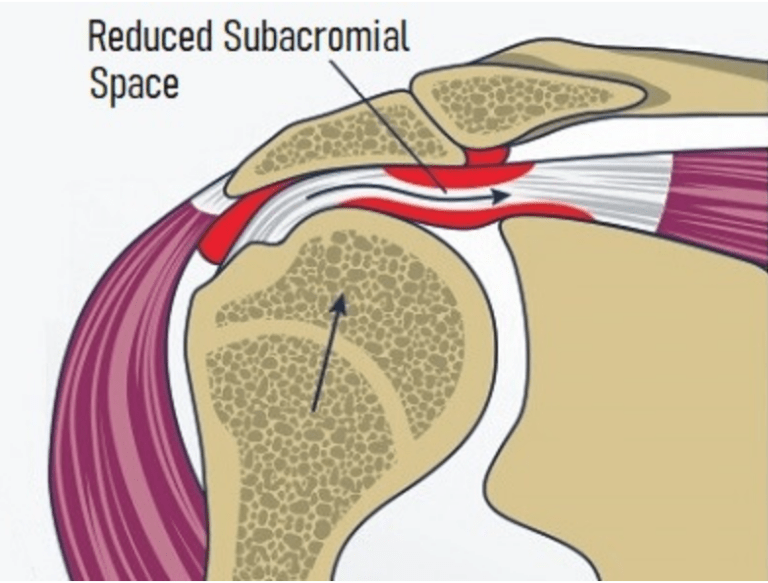
(Image Credit: https://www.shoulder-pain-explained.com)
The logic is that the tendons and other tissues inside the space get damaged when pinched between the arm bone and acromion. This has led to many treatments designed to maintain the subacromial space, including exercise and even removing the bony ceiling.
WHY SOME SAY IMPINGEMENT IS WRONG
So this whole time we’ve been blaming the acromion for most shoulder pain, but here’s why some are saying that’s not correct.
If you want to take a deep dive into the research, this paper by Jeremy Lewis covers it extensively. But I’ll do my best to summarize it.
1. THE WEAPON DOESN’T MATCH THE CRIME
If the primary cause of rotator cuff tears is irritation due to rubbing against the undersurface of the acromion, then most rotator cuff tears should be found on the upper part of the tendon (where it makes contact with the acromion.)
However, this isn’t necessarily the case.
The evidence shows that there is not a consistent trend for tear location. And actually, some papers show that most tears are on the articular side (or opposite side of the acromion.)
2. THE ACROMION SEEMS IRRELEVANT
One of the long-held beliefs is that some acromion shapes are more likely to cause impingement than others.
As you can see below, the nasty hooked acromion (Type III) is believed to cause more impingement issues than the safe flat one.

However, again as the paper from Lewis points out, the evidence doesn’t support this belief. In a study of over 500 people who underwent shoulder surgery, there was not a significant relationship between acromion shape and rotator cuff tears.
Even more compelling, is that removing some of the acromion to open up the space should be a slamdunk for treating impingement. But a group of people who had part of their acromion removed had no better outcomes than those who had shoulder surgery without any acromion removal.
3. IT’S NOT BLACK AND WHITE
And finally, I’ll lump a few different observations into this last clinical finding that suggests impingement syndrome is not actually the root cause of most shoulder problems.
Basically, if impingement was the primary cause of shoulder pain and degenerative rotator cuff tears, there would be more consistency among all those diagnosed.
But if you look at the research, it’s really all over the place.
For starters, there are many people with painful shoulders that don’t have anything remarkable on their imaging, while others live life pain-free with an MRI that reveals a whole lot of damage.
There is also the observation that certain postures increase the risk of impingement. And we know the common desk posture, with the back rounded forward and shoulders slouched, will narrow the subacromial space.
But again, the research does not show a clear relationship between posture and impingement syndrome.
Then lastly, there are inconsistencies in the degree of impingement and pain, and the clinical tests used to diagnose impingement are believed to be unreliable.
Basically saying that we’re just slapping a label of impingement on all shoulder pain, and this creates a psychological hurdle of a meat grinder in the shoulder that can be hard to overcome.
WHAT THE…?
After presenting the current evidence on shoulder impingement, I bet you’re wondering what you should do about your cranky shoulder. That’s especially true if you’ve been diagnosed with “shoulder impingement” by a doctor or clinician.
There is still a good amount of uncertainty around shoulder pain but, it’s evident that over the years, the acromion has gotten too much heat for shoulder pain and rotator cuff disease.
The diagnosis of shoulder impingement became a big bucket to throw general shoulder problems that didn’t meet the criteria for major things like big rotator cuff tears, labrum tears, or frozen shoulder.
This has likely led to some problems treating shoulder pain. Here are what I believe are fair conclusions about the current state of shoulder impingement and what it means for shoulder pain rehab.
Unnecessary Surgeries
For starters, treating impingement has led to many surgeries that weren’t totally necessary. More and more evidence is coming out to show that shaving or cutting out the acromion isn’t all that helpful for general shoulder pain.
That means unnecessary risks, costs, and added recovery times to get to the bottom of a shoulder problem.
There are outliers that do require surgery on the acromion, still, the big take-home is that the conservative approach works for most without cutting the acromion, and it should be the first option for treating this thing we call “impingement.”
However, for that to be successful, it requires complete buy-in from both the patient and clinician.
It May Inhibit Healing
It feels good to have a culprit. It imposes blame on an underlying problem that points towards a potential fix. But blaming the acromion for shoulder pain may cause more harm than good.
Check out our latest post on the problem with nocebos for more on the physical harm that our psychology may cause.
The summary of nocebo is that it builds an insidious belief that a bone is grinding away at one’s rotator cuff, which doesn’t give them hope that their pain will disappear without fixing that problem.
So the critical message here is that the tendons naturally slide between the bones, and “impingement” is normal and shouldn’t be of concern. But if your tendon is pissed off, it will let you know, especially when pulled on or compressed.
And the good news is, the gradual strengthening of the tendons and muscles works if you give it time.
Missing The Big Picture
The narrative of impingement is also a distraction from other underlying problems that need to be addressed.
It’s not just your anatomy, but a disorder that can be driven by a number of things.
When the tissues of the injured tendon are examined closer, it reveals a tendon that has poor circulation, weakly organized fibers, and a relatively low level of inflammation.
Tendons weaken and break down without proper stimulus, leading to decreased joint function and mobility.
So rather than building fear of movement, there needs to be a better push to load tendons to stay healthy. Exercise and strengthening aren’t just for weight loss and beach bodies, but when dosed correctly, they can also lead to improvements in joint health that support active living for a lifetime.
Save Your Shoulders
“Impingement” is a condition that we’ve likely misunderstood.
We can reduce the occurrence and successfully treat it with exercise, but only when it’s taken seriously.
If you’re dealing with impingement, give physical therapy your all and you should see great results.
But, remember to keep up your routine even after you feel better; this will help ensure your shoulder stays healthy for years to come.